Introduction to the Cardiovascular System
The heart is the life-giving, ever-beating muscle in your chest. From inside the womb until death, the thump goes on. The heart for the average human will contract about 3 billion times; never resting, never stopping to take a break except for a fraction of a second between beats. At 80 years of age, a person’s heart will continue to beat an average of 100,000 times a day. Many believe that the heart is the first organ to become functional. Within weeks of conception the heart starts its mission of supplying the body with nutrients even though the embryo is no bigger than a capital letter on this page. The primary function of the heart is to pump blood through the arteries, capillaries, and veins. There are an estimated 60,000 miles of vessels throughout an adult body. Blood transports oxygen, nutrients, disease causing viruses, bacteria, hormones and has other important functions as well. The heart is the pump that keeps blood circulating properly. Americans today have many options to take care of their heart and circulatory system. Expanding medical technology has made it much easier to do so. This chapter is dedicated to the heart and its many parts.
The Heart
The heart is a hollow, muscular organ about the size of a fist. It is responsible for pumping blood through the blood vessels by repeated, rhythmic contractions. The heart is composed of cardiac muscle, an involuntary muscle tissue that is found only within this organ. The term “cardiac” (as in cardiology) means “related to the heart” and comes from the Greek word kardia, for “heart.” It has a four-chambered, double pump and is located in the thoracic cavity between the lungs. The cardiac muscle is self-exciting, meaning it has its own conduction system. This is in contrast with skeletal muscle, which requires either conscious or reflex nervous stimuli. The heart’s rhythmic contractions occur spontaneously, although the frequency or heart rate can be changed by nervous or hormonal influence such as exercise or the perception of danger.
Endocardium
The endocardium is the innermost lining of the heart which consists of the endothelial cells forming a smooth membrane in places, and a pocked and tribeculated surface in others (mainly the ventricles, or lower pumping chambers).
Myocardium
The myocardium is the muscular tissue of the heart. The myocardium is composed of specialized cardiac muscle cells with an ability not possessed by muscle tissue elsewhere in the body. Cardiac muscle, like other muscles, can contract, but it can also conduct electricity, like nerves. The blood to the myocardium is supplied by the coronary arteries. If these arteries are occluded by atherosclerosis and/or thrombosis, this can lead to angina pectoris or myocardial infarction due to ischemia (lack of oxygen). Failure of the heart to contract properly (for various reasons) is termed heart failure, generally leading to fluid retention, edema, pulmonary edema, renal insufficiency, hepatomegaly, a shortened life expectancy and decreased quality of life.
Epicardium
The outer most layer next to the myocardium is known as the Epicardium. This is the outer layer after endocardium and myocardium that consists of a thin layer of connective tissue and fat.
Pericardium
The pericardium is the thick, membranous sac that surrounds the heart. It protects and lubricates the heart. There are two layers to the pericardium: the fibrous pericardium and the serous pericardium. The serous pericardium is divided into two layers; in between these two layers there is a space called the pericardial cavity.
Heart Chambers
The heart has four chambers, two atria and two ventricles. The atria are smaller with thin walls, while the ventricles are larger and much stronger.
Atrium
There are two atria on either side of the heart. On the right side is the atrium that contains blood which is poor in oxygen. The left atrium contains blood which has been oxygenated and is ready to be sent to the body. The right atrium receives de-oxygenated blood from the superior vena cava and inferior vena cava. The left atrium receives oxygenated blood from the left and right pulmonary veins. Atria facilitate circulation primarily by allowing
uninterrupted venous flow to the heart, preventing the inertia of interrupted venous flow that would otherwise occur at each ventricular systole.
Ventricles
The ventricle is a heart chamber which collects blood from an atrium and pumps it out of the heart. There are two ventricles: the right ventricle pumps blood into the pulmonary circulation for the lungs, and the left ventricle pumps blood into the systemic circulation for the rest of the body. Ventricles have thicker walls than the atria, and thus can create the higher blood pressure. Comparing the left and right ventricle, the left ventricle has thicker walls because it needs to pump blood to the whole body. This leads to the common misconception that the heart lies on the left side of the body.
Septum
The interventricular septum (ventricular septum, or during development septum inferius) is the thick wall separating the lower chambers (the ventricles) of the heart from one another. The ventricular septum is directed backward and to the right, and is curved toward the right ventricle. The greater portion of it is thick and muscular and constitutes the muscular ventricular septum. Its upper and posterior part, which separates the aortic vestibule from the lower part of the right atrium and upper part of the right ventricle, is thin and fibrous, and is termed the membranous ventricular septum.
Valves
The two atrioventricular (AV) valves are one-way valves that ensure that blood flows from the atria to the ventricles, and not the other way. The two semilunar (SL) valves are present in the arteries leaving the heart; they prevent blood from flowing back into the ventricles. The sound heard in a heart beat is the heart valves shutting. The right AV valve is also called the tricuspid valve because it has three flaps. It is located between the right atrium and the right ventricle. The tricuspid valve allows blood to flow from the right atrium into the right ventricle when the heart is relaxed during diastole. When the heart begins to contract, the heart enters a phase called systole, and the atrium pushes blood into the ventricle. Then, the ventricle begins to contract and blood pressure inside the heart rises. When the ventricular pressure exceeds the pressure in the atrium, the tricuspid valve snaps shut. The left AV valve is also called the bicuspid valve because it has two flaps. It is also known as the mitral valve due to the resemblance to a bishop’s mitre (liturgical headdress). This valve prevents blood in the left ventricle from flowing into the left atrium. As it is on the left side of the heart, it must withstand a great deal of strain and pressure; this is why it is made of only two cusps, as a simpler mechanism entails a reduced risk of malfunction. There are two remaining valves called the Semilunar Valves. They have flaps that resemble half moons. The pulmonary semilunar valve lies between the right ventricle and the pulmonary trunk. The aortic semilunar valve is located between the ventricle and the aorta.
Subvalvular Apparatus
The chordae tendinae are attached to papillary muscles that cause tension to better hold the valve. Together, the papillary muscles and the chordae tendinae are known as the subvalvular apparatus. The function of the subvalvular apparatus is to keep the valves from prolapsing into the atria when they close. The subvalvular apparatus have no effect on the opening and closing of the valves. This is caused entirely by the pressure gradient across the valve.
Complications with the Heart
The most common congenital abnormality of the heart is the bicuspid aortic valve. In this condition, instead of three cusps, the aortic valve has two cusps. This condition is often undiagnosed until the person develops calcific aortic stenosis. Aortic stenosis occurs in this condition usually in patients in their 40s or 50s, an average of 10 years earlier than in people with normal aortic valves. Another common complication of rheumatic fever is thickening and stenosis (partial blocking) of the mitral valve. For patients who have had rheumatic fever dentists are advised to prophylactally administer antibiotics prior to dental work to
prevent bacterial endocarditis that occurs when bacteria from the teeth enter the circulation
and attach to damaged heart valves. The aortic valve is a semilunar valve, but it´s called bicuspid because of it´s regular three “cusps” or “semilunar” valves, and is not to be confused with the left atrioventricular valve, which is more commonly called the mitral valve, and is one of the two cuspidal valves.
Passage of Blood Through the Heart
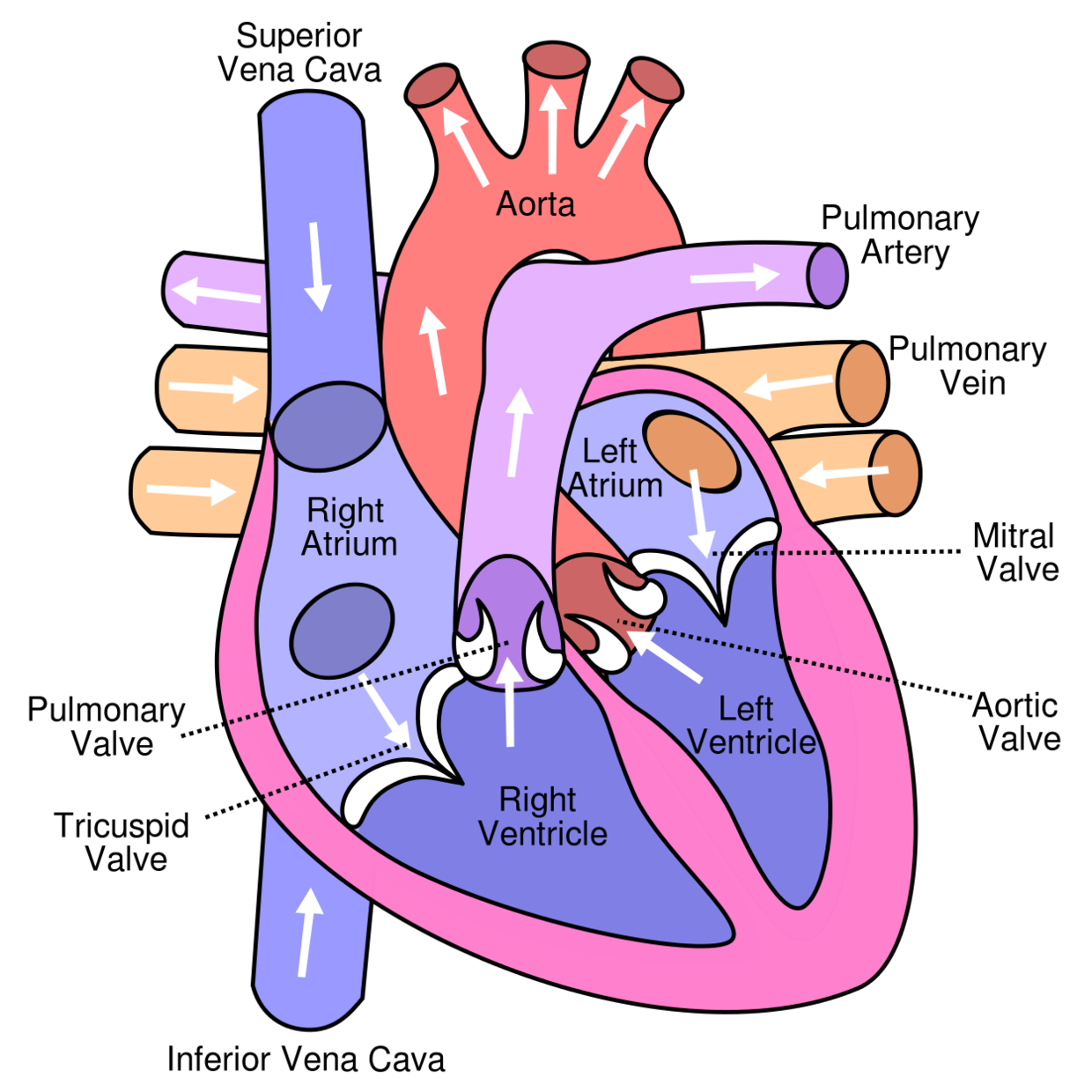
Diagram of the human heart
While it is convenient to describe the flow of the blood through the right side of the heart and then through the left side, it is important to realize that both atria contract at the same time and that both ventricles contract at the same time. The heart works as two pumps, one on the right and one on the left that works simultaneously. The right pump pumps the blood to the lungs or the pulmonary circulation at the same time that the left pump pumps blood to the rest of the body or the systemic circulation. Venous blood from systemic circulation (deoxygenated) enters the right atrium through the superior and inferior vena cava. The right atrium contracts and forces the blood through the tricuspid valve (right atrioventricular valve) and into the right ventricles. The right ventricles contract and force the blood through the pulmonary semilunar valve into the pulmonary trunk and out the pulmonary artery. This takes the blood to the lungs where the blood releases carbon dioxide and receives a new supply of oxygen. The new blood is carried in the pulmonary veins that take it to the left atrium. The left atrium then contracts and forces blood through the left atrioventricular, bicuspid, or mitral, valve into the left ventricle. The left ventricle contracts forcing blood through the aortic semilunar valve into the ascending aorta. It then branches to arteries carrying oxygen rich blood to all parts of the body.
Blood Flow After the Heart
Aorta-Arteries-Arterioles-Capillaries-Venules-Veins-Vena Cava
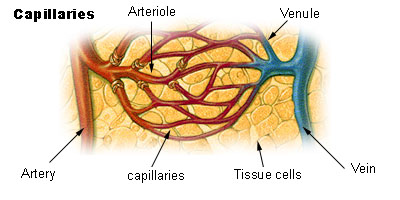
Blood Flow Through Capillaries
From the arterioles, the blood then enters one or more capillaries. The walls of capillaries are so thin and fragile that blood cells can only pass in single file. Inside the capillaries, exchange of oxygen and carbon dioxide takes place. Red blood cells inside the capillary releases their oxygen which passes through the wall and into the surrounding tissue. The tissue then releases waste, such as carbon dioxide, which then passes through the wall and into the red blood cells.
The Circulatory System
The circulatory system is extremely important in sustaining life. It’s proper functioning is responsible for the delivery of oxygen and nutrients to all cells, as well as the removal of carbon dioxide, waste products, maintenance of optimum pH, and the mobility of the elements, proteins and cells, of the immune system. In developed countries, the two leading causes of death, myocardial infarction and stroke are each direct results of an arterial system that has been slowly and progressively compromised by years of deterioration.
Arteries
Arteries are muscular blood vessels that carry blood away from the heart, oxygenated and deoxygenated blood . The pulmonary arteries will carry deoxygenated blood to the lungs and the sytemic arteries will carry oxygenated blood to the rest of the body. Arteries have a thick wall that consists of three layers. The inside layer is called the endothelium, the middle layer is mostly smooth muscle and the outside layer is connective tissue. The artery walls are thick so that when blood enters under pressure the walls can expand.
Arterioles
An arteriole is a small artery that extends and leads to capillaries. Arterioles have thick smooth muscular walls. These smooth muscles are able to contract (causing vessel constriction) and relax (causing vessel dilation). This contracting and relaxing affects blood pressure; the higher number of vessels dilated, the lower blood pressure will be. Arterioles are just visible to the naked eye.
Capillaries
Capillaries are the smallest of a body’s vessels; they connect arteries and veins, and most closely interact with tissues. They are very prevalent in the body; total surface area is about 6,300 square meters. Because of this, no cell is very far from a capillary, no more than 50 micrometers away. The walls of capillaries are composed of a single layer of cells, the endothelium, which is the inner lining of all the vessels. This layer is so thin that molecules such as oxygen, water and lipids can pass through them by diffusion and enter the tissues. Waste products such as carbon dioxide and urea can diffuse back into the blood to be carried away for removal from the body. The “capillary bed” is the network of capillaries present throughout the body. These beds are able to be “opened” and “closed” at any given time, according to need. This process is called autoregulation and capillary beds usually carry no more than 25% of the amount of blood it could hold at any time. The more metabolically active the cells, the more capillaries it will require to supply nutrients.
Veins
Veins carry blood to the heart. The pulmonary veins will carry oxygenated blood to the heart awhile the systemic veins will carry deoxygenated to the heart. Most of the blood volume is found in the venous system; about 70% at any given time. The veins outer walls have the same three layers as the arteries, differing only because there is a lack of smooth muscle in the inner layer and less connective tissue on the outer layer. Veins have low blood pressure compared to arteries and need the help of skeletal muscles to bring blood back to the heart. Most veins have one-way valves called venous valves to prevent backflow caused by gravity. They also have a thick collagen outer layer, which helps maintain blood pressure and stop blood pooling. If a person is standing still for long periods or is bedridden, blood can accumulates in veins and can cause varicose veins. The hollow internal cavity in which the blood flows is called the lumen. A muscular layer allows veins to contract, which puts more blood into circulation. Veins are used medically as points of access to the blood stream, permitting the withdrawal of blood specimens (venipuncture) for testing purposes, and enabling the infusion of fluid, electrolytes, nutrition, and medications (intravenous delivery).
Venules
A venule is a small vein that allows deoxygenated blood to return from the capillary beds to the larger blood veins, except in the pulmonary circuit were the blood is oxygenated. Venules have three layers; they have the same makeup as arteries with less smooth muscle, making them thinner.
The Cardiovascular Pathways

Human circulatory system. Arteries are shown in red, veins blue.
The double circulatory system of blood flow refers to the separate systems of pulmonary circulation and the systemic circulation in amphibians, birds and mammals (including humans.) In contrast, fishes have a single circulation system. For instance, the adult human heart consists of two separated pumps, the right side with the right atrium and ventricle (which pumps deoxygenated blood into the pulmonary circulation), and the left side with the left atrium and ventricle (which pumps oxygenated blood into the systemic circulation). Blood in one circuit has to go through the heart to enter the other circuit. Blood circulates through the body two to three times every minute. In one day, the blood travels a total of 19,000 km (12,000 miles), or four times the distance across the U.S. from coast to coast.
The Pulmonary Circuit
In the pulmonary circuit, blood is pumped to the lungs from the right ventricle of the heart. It is carried to the lungs via pulmonary arteries. At lungs, oxygen in the alveolae diffuses to the capillaries surrounding the alveolae and carbon dioxide inside the blood diffuses to the alveolae. As a result, blood is oxygenated which is then carried to the heart’s left half -to the left atrium via pulmonary veins. Oxygen rich blood is prepared for the whole organs
and tissues of the body. This is important because mitochondria inside the cells should use oxygen to produce energy from the organic compounds.
The Systemic Circuit
The systemic circuit supplies oxygenated blood to the organ system. Oxygenated blood from the lungs is returned to the left atrium, then the ventricle contracts and pumps blood into the aorta. Systemic arteries split from the aorta and direct blood into the capillaries. Cells consume the oxygen and nutrients and add carbon dioxide, wastes, enzymes and hormones. The veins drain the deoxygenated blood from the capillaries and return the blood to the right atrium.
Aorta
The aorta is the largest of the arteries in the systemic circuit. The blood is pumped from the left ventricle into the aorta and from there it branches to all parts of the body. The aorta is an elastic artery, and as such is able to distend. When the left ventricle contracts to force blood into the aorta, the aorta expands. This stretching gives the potential energy that will help maintain blood pressure during diastole, as during this time the aorta contracts passively.
Superior Venae Cavae
The superior vena cava (SVC) is a large but short vein that carries de-oxygenated blood from the upper half of the body to the heart’s right atrium. It is formed by the left and right brachiocephalic veins (also referred to as the innominate veins) which receive blood from the upper limbs and the head and neck. The azygous vein (which receives blood from the ribcage) joins it just before it enters the right atrium.
Inferior Venae Cavae
The inferior vena cava (or IVC) is a large vein that carries de-oxygenated blood from the lower half of the body into the heart. It is formed by the left and right common iliac veins and transports blood to the right atrium of the heart. It is posterior to the abdominal cavity,
and runs along side of the vertebral column on its right side.
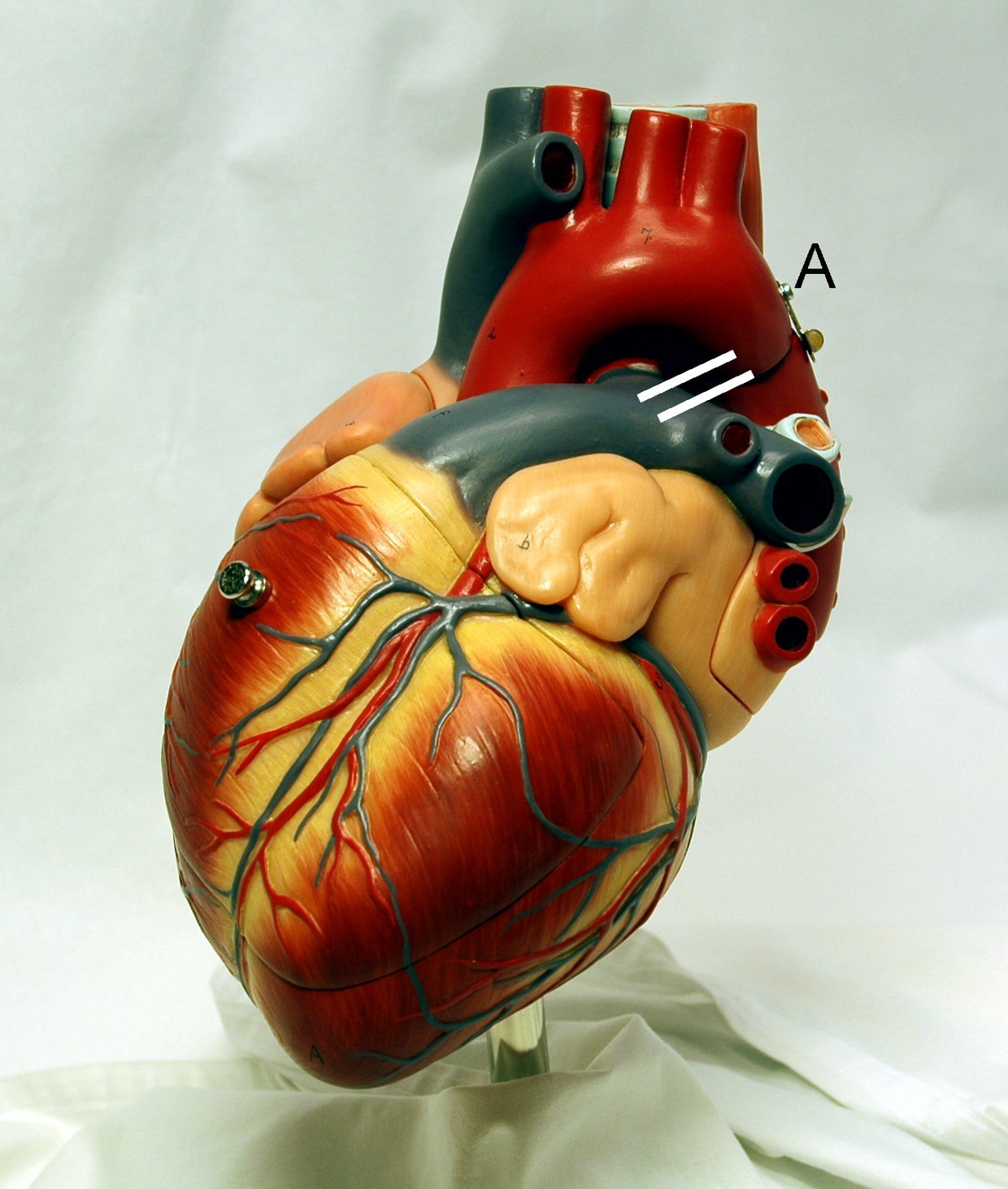
Coronary Arteries

Heart showing the Coronary Arteries
Heart showing the Coronary Arteries The coronary circulation consists of the blood vessels that supply blood to, and remove blood from, the heart muscle itself. Although blood fills the chambers of the heart, the muscle tissue of the heart, or myocardium, is so thick that it requires coronary blood vessels to deliver blood deep into the myocardium. The vessels that supply blood high in oxygen to the myocardium are known as coronary arteries. The vessels that remove the deoxygenated blood from the heart muscle are known as cardiac veins. The coronary arteries that run on the surface of the heart are called epicardial coronary arteries. These arteries, when healthy, are capable of auto regulation to maintain coronary blood flow at levels appropriate to the needs of the heart muscle. These relatively narrow vessels are commonly affected by atherosclerosis and can become blocked, causing angina or a heart attack. The coronary arteries are classified as “end circulation”, since they represent the only source of blood supply to the myocardium: there is very little redundant blood supply, which is why blockage of these vessels can be so critical. In general there are two main coronary arteries, the left and right. • Right coronary artery • Left coronary artery Both of these arteries originate from the beginning (root) of the aorta, immediately above the aortic valve. As discussed below, the left coronary artery originates from the left aortic sinus, while the right coronary artery originates from the right aortic sinus. Four percent of people have a third, the posterior coronary artery. In rare cases, a patient will have one coronary artery that runs around the root of the aorta.
Hepatic Veins
In human anatomy, the hepatic veins are the blood vessels that drain de-oxygenated blood from the liver and blood cleaned by the liver (from the stomach, pancreas, small intestine and colon) into the inferior vena cava. They arise from the substance of the liver, more specifically the central vein of the liver lobule. They can be differentiated into two groups, the upper group and lower group. The upper group of three typically arises from the posterior aspect of the liver and drain the quadrate lobe and left lobe. The lower group rise from the right lobe and caudate lobe, are variable in number, and are typically smaller than those in the upper group. None of the hepatic veins have valves.
Cardiac Cycle
Cardiac cycle is the term used to describe the relaxation and contraction that occur, as a heart works to pump blood through the body. Heart rate is a term used to describe the frequency of the cardiac cycle. It is considered one of the four vital signs. Usually it is calculated as the number of contractions (heart beats) of the heart in one minute and expressed as “beats per minute” (bpm). When resting, the adult human heart beats at about 70 bpm (males) and 75 bpm (females), but this rate varies between people. However, the reference range is nominally between 60 bpm (if less termed bradycardia) and 100 bpm (if greater, termed tachycardia). Resting heart rates can be significantly lower in athletes, and significantly higher in the obese. The body can increase the heart rate in response to a wide variety of conditions in order to increase the cardiac output (the amount of blood ejected by
the heart per unit time). Exercise, environmental stressors or psychological stress can cause the heart rate to increase above the resting rate. The pulse is the most straightforward way of measuring the heart rate, but it can be deceptive when some strokes do not lead to much cardiac output. In these cases (as happens in some arrhythmias), the heart rate may be considerably higher than the pulse. Every single ‘beat’ of the heart involves three major stages: atrial systole, ventricular systole and complete cardiac diastole. Throughout the cardiac cycle, the blood pressure increases and decreases. As ventricles contract the pressure rise, causing the AV valves to slam shut.
Systole

The heart in the systole phase.
The heart in the systole phase. Systole, or contraction, of the heart is initiated by the electrical cells of the sinoatrial node, which is the heart’s natural pacemaker. These cells are activated spontaneously by depolarization of their membranes beyond a certain threshold for excitation. At this point, voltage-gated calcium channels on the cell membrane open and allow calcium ions to pass through, into the sarcoplasm, or interior, of the muscle cell. Some calcium ions bind to receptors on the sarcoplasmic reticulum causing an influx of calcium ions into the sarcoplasm. The calcium ions bind to the troponin, causing a conformation change, breaking the bond between the protein tropomyosin, to which the troponin is attached, and the myosin binding sites. This allows the myosin heads to bind to the myosin binding sites on the actin protein filament and contraction results as the myosin heads draw the actin filaments along, are bound by ATP, causing them to release the actin, and return to their original position, breaking down the ATP into ADP and a phosphate group. The action potential spreads via the passage of sodium ions through the gap junctions that connect the sarcoplasm of adjacent myocardial cells. Norepinephrine (noradrenaline) is released by the terminal boutons of depolarized sympathetic fibers, at the sinoatrial and atrioventricular nodes. Norepinephrine diffuses across the synaptic cleft binds to the β1-adrenoreceptors – G-protein linked receptors, consisting of seven transmembrane domains – shifting their equilibrium towards the active state. The receptor changes its conformation and mechanically activates the G-protein which is released. The G-protein is involved in the production of adenosine 3′,5′-cyclic monophosphate (cAMP) from adenosine triphosphate (ATP) and this in turn activates the protein kinase (β-adrenoreceptor kinase). β-adrenoreceptor kinase phosphorylates the calcium ion channels in the sarcolemma, so that calcium ion influx is increased when they are activated by the appropriate transmembrane voltage. This will of course, cause more of the calcium receptors in the sarcoplasmic reticulum to be activated, creating a larger flow of calcium ions into the sarcoplasm. More troponin will be bound and more myosin binding sites cleared [of tropomyosin] so that more myosin heads can be recruited for the contraction and a greater force and speed of contraction results. [Phosphodiesterase catalyses the decomposition of cAMP to AMP so that it is no longer able to activate the protein kinase. AMP will of course, go on to be phosphorylated to ATP and may be recycled.] Noradrenaline also affects the atrioventricular node, reducing the delay before continuing conduction of the action potential via the bundle of HIS.
Diastole
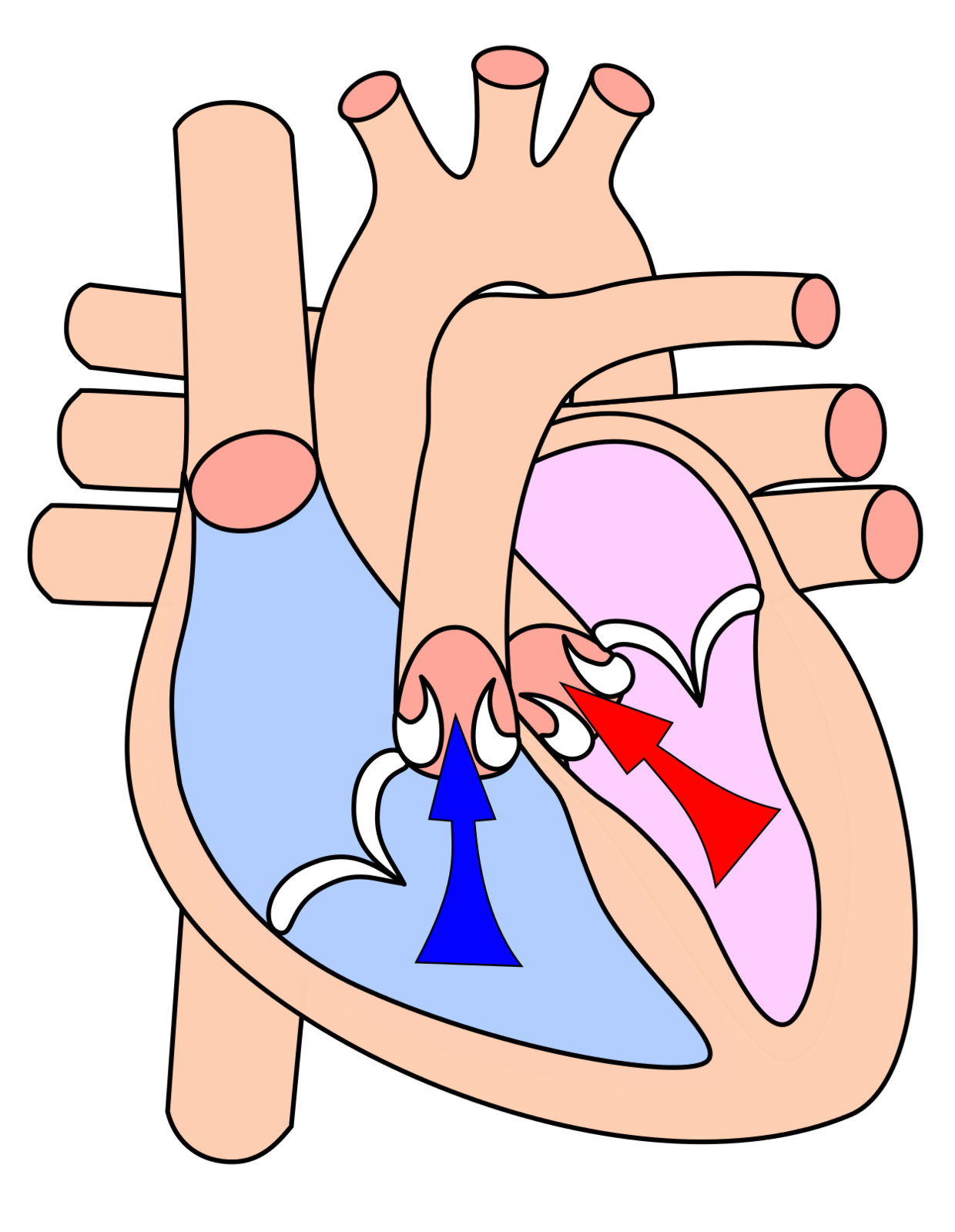
The heart in the diastole phase.
The heart in the diastole phase. Cardiac Diastole is the period of time when the heart relaxes after contraction in preparation for refilling with circulating blood. Ventricular diastole is when the ventricles are relaxing, while atrial diastole is when the atria are relaxing. Together they are known as complete cardiac diastole. It should be noted that even this relaxation is an active, energy-spending process. During ventricular diastole, the pressure in the (left and right) ventricles drops from the peak that it reaches in systole. When the pressure in the left ventricle drops to below the pressure in the left atrium, the mitral valve opens, and the left ventricle fills with blood that was accumulating in the left atrium. Likewise, when the pressure in the right ventricle drops below that in the right atrium, the tricuspid valve opens and the right ventricle fills with blood that was in the right atrium.
“Lub-Dub”
The first heart tone, or S1, “Lub” is caused by the closure of the atrioventricular valves, mitral and tricuspid, at the beginning of ventricular contraction, or systole. When the pressure in the ventricles rises above the pressure in the atria, these valves close to prevent regurgitation of blood from the ventricles into the atria. The second heart tone, or S2 (A2 and P2), “Dub” is caused by the closure of the aortic valve and pulmonic valve at the end of ventricular systole. As the left ventricle empties, its pressure falls below the pressure in the aorta, and the aortic valve closes. Similarly, as the pressure in the right ventricle falls below the pressure in the pulmonary artery, the pulmonic valve closes. During inspiration, negative intrathoracic pressure causes increased blood return into the right side of the heart. The increased blood volume in the right ventricle causes the pulmonic valve to stay open longer during ventricular systole. This causes an increased delay in the P2 component of S2. During expiration, the positive intrathoracic pressure causes decreased blood return to the right side of the heart. The reduced volume in the right ventricle allows the pulmonic valve to close earlier at the end of ventricular systole, causing P2 to occur earlier, and “closer” to A2. It is physiological to hear the splitting of the second heart tone by younger people and during inspiration. During expiration normally the interval between the two components shortens and the tone becomes merged.
Source: Cray MI, Ch. 7 The Cardiovascular System,Textbook of Human Physiology and Biophysics, V#1. Atlanta Ga: IVMS 2014:179-93
