Introduction to the Urinary System

The Urinary System is a group of organs in the body concerned with filtering out excess fluid and other substances from the bloodstream. The substances are filtered out from the body in the form of urine. Urine is a liquid produced by the kidneys, collected in the bladder and excreted through the urethra. Urine is used to extract excess minerals or vitamins as well as blood corpuscles from the body. The Urinary organs include the kidneys, ureters, bladder, and urethra. The Urinary system works with the other systems of the body to help maintain homeostasis. The kidneys are the main organs of homeostasis because they maintain the acid base balance and the water salt balance of the blood.
Functions of the Urinary System
One of the major functions of the Urinary system is the process of excretion. Excretion is the process of eliminating, from an organism, waste products of metabolism and other materials that are of no use. The urinary system maintains an appropriate fluid volume by regulating the amount of water that is excreted in the urine. Other aspects of its function includeregulating the concentrations of various electrolytes in the body fluids and maintaining normal pH of the blood. Several body organs carry out excretion, but the kidneys are the most important excretory organ. The primary function of the kidneys is to maintain a stable internal environment (homeostasis) for optimal cell and tissue metabolism. They do this by separating urea, mineral salts, toxins, and other waste products from the blood. They also do the job of conserving water, salts, and electrolytes. At least one kidney must function properly for life to be maintained.
Six important roles of the kidneys are:
1. Regulation of plasma ionic composition. Ions such as sodium, potassium, calcium, magnesium, chloride, bicarbonate, and phosphates are regulated by the amount that the kidney excretes.
2. Regulation of plasma osmolarity. The kidneys regulate osmolarity because they have direct control over how many ions and how much water a person excretes.
3. Regulation of plasma volume. Your kidneys are so important they even have an effect on your blood pressure. The kidneys control plasma volume by controlling how much water a person excretes. The plasma volume has a direct effect on the total blood volume, which has a direct effect on your blood pressure. Salt(NaCl)will cause osmosis to happen; the diffusion of water into the blood.
4. Regulation of plasma hydrogen ion concentration (pH).The kidneys partner up with the lungs and they together control the pH. The kidneys have a major role because they control the amount of bicarbonate excreted or held onto. The kidneys help maintain the blood Ph mainly by excreting hydrogen ions and reabsorbing bicarbonate ions as needed.
5. Removal of metabolic waste products and foreign substances from the plasma. One of the most important things the kidneys excrete is nitrogenous waste. As the liver breaks down amino acids it also releases ammonia. The liver then quickly combines that ammonia with carbon dioxide, creating urea which is the primary nitrogenous end product of metabolism in humans. The liver turns the ammonia into urea because it is much less toxic. We can also excrete some ammonia, creatinine and uric acid. The creatinine comes from the metabolic breakdown of creatine phospate (a high-energy phosphate in muscles). Uric acid comes from the break down of nucleotides. Uric acid is insoluble and too much uric acid in the blood will build up and form crystals that can collect in the joints and cause
gout.
6. Secretion of Hormones The endocrine system has assistance from the kidney’s when releasing hormones. Renin is released by the kidneys. Renin leads to the secretion of aldosterone which is released from the adrenal cortex. Aldosterone promotes the kidneys. to reabsorb the sodium (Na+) ions. The kidneys also secrete erythropoietin when the blood doesn’t have the capacity to carry oxygen. Erythropoietin stimulates red blood cell production. The Vitamin D from the skin is also activated with help from the kidneys. Calcium (Ca+) absorption from the digestive tract is promoted by vitamin D.
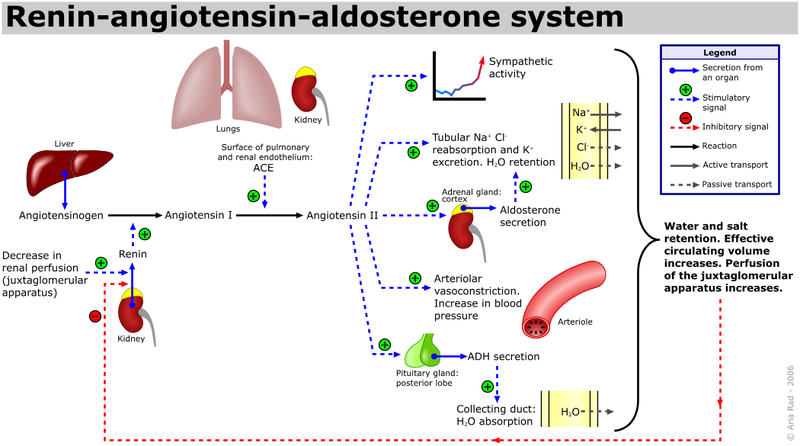
RAAS
Organs in the Urinary System
Kidneys And Their Structure
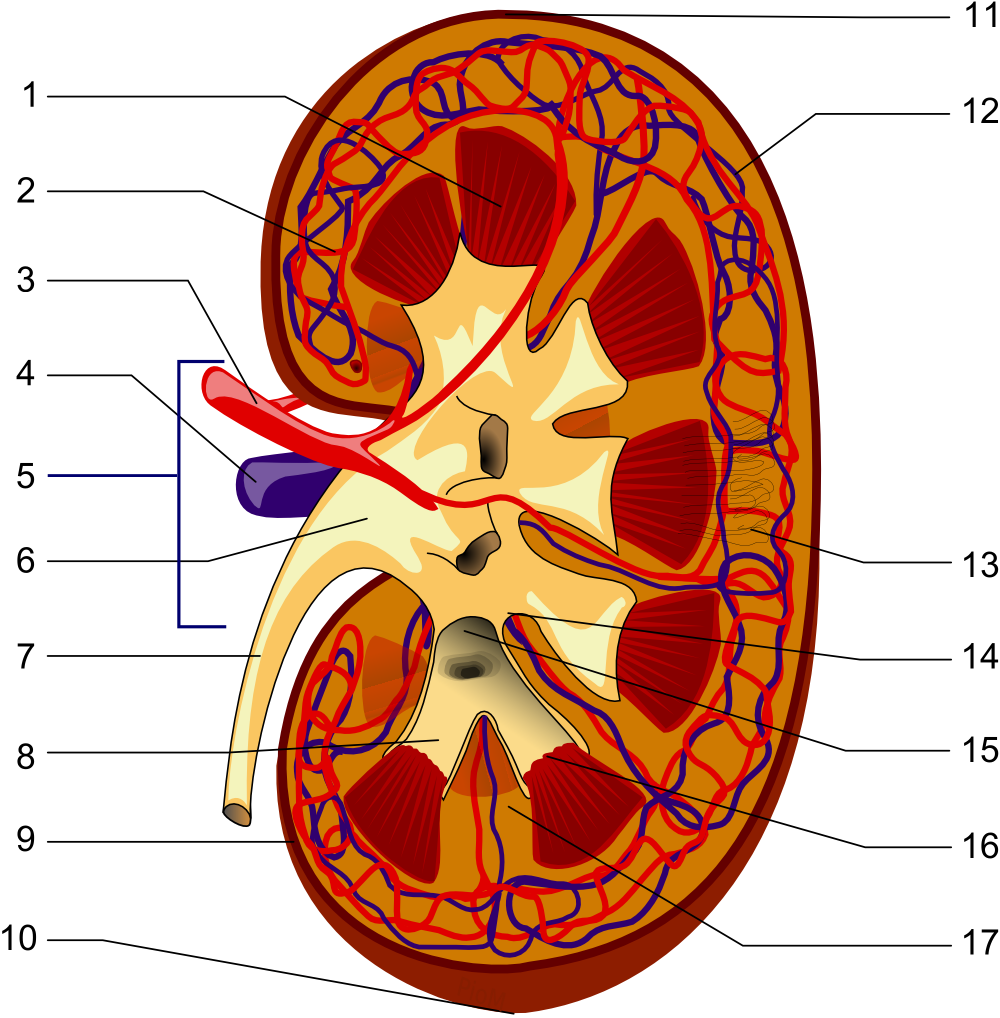
1. Renal pyramid 2. Interlobar artery 3. Renal artery 4. Renal vein 5. Renal hylum 6. Renal pelvis 7. Ureter 8. Minor calyx 9. Renal capsule 10. Inferior renal capsule 11. Superior renal capsule 12. Interlobar vein 13. Nephron 14.Minor calyx 15. Major calyx 16. Renal papilla 17. Renal column
The kidneys are a pair of bean shaped, brown organs about the size of your fist.It measures 10-12 cm long. They are covered by the renal capsule, which is a tough capsule of fibrous connective tissue. Adhering to the surface of each kidney is two layers of fat to help cushion them. There is a concaved side of the kidney that has a depression where a renal artery enters, and a renal vein and a ureter exit the kidney. The kidneys are located at the rear wall of the abdominal cavity just above the waistline, and are protected by the ribcage. They are considered retroperitoneal, which means they lie behind the peritoneum. There are three major regions of the kidney, renal cortex, renal medulla and the renal pelvis. The outer, granulated layer is the renal cortex. The cortex stretches down in between a radially striated inner layer. The inner radially striated layer is the renal medulla. This contains pyramid shaped tissue called the renal pyramids, separated by renal columns. The ureters are continuous with the renal pelvis and is the very center of the kidney.
Renal Vein
The renal veins are veins that drain the kidney. They connect the kidney to the inferior vena cava. Because the inferior vena cava is on the right half of the body, the left renal vein is generally the longer of the two. Unlike the right renal vein, the left renal vein often receives the left gonadal vein (left testicular vein in males, left ovarian vein in females). It frequently receives the left suprarenal vein as well.
Renal Artery
The renal arteries normally arise off the abdominal aorta and supply the kidneys with blood. The arterial supply of the kidneys are variable and there may be one or more renal arteries supplying each kidney. Due to the position of the aorta, the inferior vena cava and the kidneys in the body, the right renal artery is normally longer than the left renal artery. The right renal artery normally crosses posteriorly to the inferior vena cava. The renal arteries carry a large portion of the total blood flow to the kidneys. Up to a third of the total cardiac output can pass through the renal arteries to be filtered by the kidneys.
Ureters
The ureters are two tubes that drain urine from the kidneys to the bladder. Each ureter is a muscular tube about 10 inches (25 cm) long. Muscles in the walls of the ureters send the urine in small spurts into the bladder, (a collapsible sac found on the forward part of the cavity of the bony pelvis that allows temporary storage of urine). After the urine enters the bladder from the ureters, small folds in the bladder mucosa act like valves preventing backward flow of the urine. The outlet of the bladder is controlled by a sphincter muscle. A full bladder stimulates sensory nerves in the bladder wall that relax the sphincter and allow release of the urine. However, relaxation of the sphincter is also in part a learned response under voluntary control. The released urine enters the urethra.
Urinary Bladder
The urinary bladder is a hollow, muscular and distendible or elastic organ that sits on the pelvic floor (superior to the prostate in males). On its anterior border lies the pubic symphysis and, on its posterior border, the vagina (in females) and rectum (in males). The urinary bladder can hold approximately 17 to 18 ounces (500 to 530 ml) of urine, however the desire to micturate is usually experienced when it contains about 150 to 200 ml. When the bladder fills with urine (about half full), stretch receptors send nerve impulses to the spinal cord, which then sends a reflex nerve impulse back to the sphincter (muscular valve) at the neck of the bladder, causing it to relax and allow the flow of urine into the urethra. The Internal urethral sphincter is involuntary. The ureters enter the bladder diagonally from its dorsolateral floor in an area called the trigone. The trigone is a triangular shaped area on the postero-inferior wall of the bladder. The urethra exits at the lowest point of the triangle of the trigone. The urine in the bladder also helps regulate body temperature. A bladder when operating normally empties completely upon a complete discharge, otherwise it is a sign that its elasticity is compromised, when it becomes completely void of fluid, it may cause a chilling sensation due to the rapid change of body temperature.
Urethra

Female urethra (labeled at bottom right.)
The urethra is a muscular tube that connects the bladder with the outside of the body. The function of the urethra is to remove urine from the body. It measures about 1.5 inches (3.8 cm) in a woman but up to 8 inches (20 cm) in a man. Because the urethra is so much shorter in a woman it makes it much easier for a woman to get harmful bacteria in her bladder this is commonly called a bladder infection or a UTI. The most common bacteria of a UTI is E-coli from the large intestines that have been excreted in fecal matter. Female urethra In the human female, the urethra is about 1-2 inches long and opens in the vulva between the clitoris and the vaginal opening. Men have a longer urethra than women. This means that women tend to be more susceptible to infections of the bladder (cystitis) and the urinary tract.
Male urethra

Male Sphincter urethrae muscle
– The male urethra laid open on its anterior
(upper) surface. (Region visible, but muscle
not labeled.)
In the human male, the urethra is about 8 inches long and opens at the end of the head of the penis. The length of a male’s urethra, and the fact it contains a number of bends, makes catheterisation more difficult. The urethral sphincter is a collective name for the muscles used to control the flow of urine from the urinary bladder. These muscles surround the urethra, so that when they contract, the urethra is closed.
• There are two distinct areas of muscle: the internal sphincter, at the bladder neck and
• the external, or distal, sphincter.
Human males have much stronger sphincter muscles than females, meaning that they can retain a large amount of urine for twice as long, as much as 800mL, i.e. “hold it”.
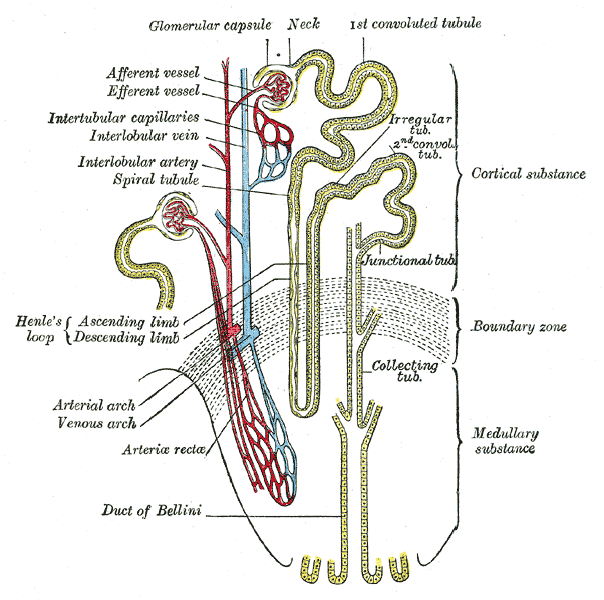
Nephrons
A nephron is the basic structural and functional unit of the kidney. The name nephron comes from the Greek word (nephros) meaning kidney. Its chief function is to regulate water and soluble substances by filtering the blood, reabsorbing what is needed and excreting the rest as urine. Nephrons eliminate wastes from the body, regulate blood volume and pressure, control levels of electrolytes and metabolites, and regulate blood pH. Its functions are vital to life and are regulated by the endocrine system by hormones such as antidiuretic hormone,
aldosterone, and parathyroid hormone. Each nephron has its own supply of blood from two capillary regions from the renal artery. Each nephron is composed of an initial filtering component (the renal corpuscle) and a tubule specialized for reabsorption and secretion (the renal tubule). The renal corpuscle filters out large solutes from the blood, delivering water and small solutes to the renal tubule for modification.
Glomerulus
The glomerulus is a capillary tuft that receives its blood supply from an afferent arteriole of the renal circulation. The glomerular blood pressure provides the driving force for fluid and solutes to be filtered out of the blood and into the space made by Bowman’s capsule. The remainder of the blood not filtered into the glomerulus passes into the narrower efferent arteriole. It then moves into the vasa recta, which are collecting capillaries intertwined with the convoluted tubules through the interstitial space, where the reabsorbed substances will also enter. This then combines with efferent venules from other nephrons into the renal vein, and rejoins with the main bloodstream.
Afferent/Efferent Arterioles
The afferent arteriole supplies blood to the glomerulus. A group of specialized cells known as juxtaglomerular cells are located around the afferent arteriole where it enters the renal corpuscle. The efferent arteriole drains the glomerulus. Between the two arterioles lies specialized cells called the macula densa. The juxtaglomerular cells and the macula densa collectively form the juxtaglomerular apparatus. It is in the juxtaglomerular apparatus cells that the enzyme renin is formed and stored. Renin is released in response to decreased blood pressure in the afferent arterioles, decreased sodium chloride in the distal convoluted
tubule and sympathetic nerve stimulation of receptors (beta-adrenic) on the juxtaglomerular cells. Renin is needed to form Angiotensin I and Angiotensin II which stimulate the secretion of aldosterone by the adrenal cortex.
Glomerular Capsule or Bowman’s Capsule
Bowman’s capsule (also called the glomerular capsule) surrounds the glomerulus and is composed of visceral (simple squamous epithelial cells) (inner) and parietal (simple squamous epithelial cells) (outer) layers. The visceral layer lies just beneath the thickened glomerular basement membrane and is made of podocytes which send foot processes over the length of the glomerulus. Foot processes interdigitate with one another forming filtration slits that, in contrast to those in the glomeruluar endothelium, are spanned by diaphragms. The size of the filtration slits restricts the passage of large molecules (eg, albumin) and cells (eg, red blood cells and platelets). In addition, foot processes have a negatively-charged coat (glycocalyx) that limits the filtration of negatively-charged molecules, such as albumin. This action is called electrostatic repulsion. The parietal layer of Bowman’s capsule is lined by a single layer of squamous epithelium. Between the visceral and parietal layers is Bowman’s space, into which the filtrate enters after passing through the podocytes’ filtration slits. It is here that smooth muscle cells and macrophages lie between the capillaries and provide support for them. Unlike the visceral layer, the parietal layer does not function in filtration. Rather, the filtration barrier is formed by three components: the diaphragms of the filtration slits, the thick glomerular basement membrane, and the glycocalyx secreted by podocytes. 99% of glomerular filtrate will ultimately be reabsorbed. The process of filtration of the blood in the Bowman’s capsule is ultrafiltration (or glomerular filtration), and the normal rate of filtration is 125 ml/min, equivalent to ten times the blood volume daily. Measuring the glomerular filtration rate (GFR) is a diagnostic test of kidney function. A decreased GFR may be a sign of renal failure. Conditions that can affect GFR include: arterial pressure, afferent arteriole constriction, efferent arteriole constriction, plasma protein concentration and colloid osmotic pressure. Any proteins that are roughly 30 kilodaltons or under can pass freely through the membrane. Although, there is some extra hindrance for negatively charged molecules due to the negative charge of the basement membrane and the podocytes. Any small molecules such as water, glucose, salt (NaCl), amino acids, and urea pass freely into Bowman’s space, but cells, platelets and large proteins do not. As a result, the filtrate leaving the Bowman’s capsule is very similar to blood plasma in composition as it passes into the proximal convoluted tubule. Together, the glomerulus and Bowman’s capsule are called the renal corpuscle.
Proximal Convoluted Tubule (PCT)
The proximal tubule can be anatomically divided into two segments: the proximal convoluted tubule and the proximal straight tubule. The proximal convoluted tubule can be divided further into S1 and S2 segments based on the histological appearance of it’s cells. Following this naming convention, the proximal straight tubule is commonly called the S3 segment. The proximal convoluted tubule has one layer of cuboidal cells in the lumen. This is the only place in the nephron that contains cuboidal cells. These cells are covered with millions of microvilli. The microvilli serve to increase surface area for reabsorption. Fluid in the filtrate entering the proximal convoluted tubule is reabsorbed into the peritubular capillaries, including approximately two-thirds of the filtered salt and water and all filtered organic solutes (primarily glucose and amino acids). This is driven by sodium transport from the lumen into the blood by the Na+/K+ ATPase in the basolateral membrane of the epithelial cells. Much of the mass movement of water and solutes occurs in between the cells through the tight junctions, which in this case are not selective. The solutes are absorbed isotonically, in that the osmotic potential of the fluid leaving the proximal tubule is the same as that of the initial glomerular filtrate. However, glucose, amino acids, inorganic phosphate, and some other solutes are reabsorbed via secondary active transport through cotransport channels driven by the sodium gradient out of the nephron.
Loop of the Nephron or Loop of Henle
The Nephron Loop or Loop of Henle.
The loop of Henle (sometimes known as the nephron loop) is a U-shaped tube that consists of a descending limb and ascending limb. It begins in the cortex, receiving filtrate from the proximal convoluted tubule, extends into the medulla, and then returns to the cortex to empty into the distal convoluted tubule. Its primary role is to concentrate the salt in the interstitium, the tissue surrounding the loop.
Descending limb
Its descending limb is permeable to water but completely impermeable to salt, and thus only indirectly contributes to the concentration of the interstitium. As the filtrate descends deeper into the hypertonic interstitium of the renal medulla, water flows freely out of the descending limb by osmosis until the tonicity of the filtrate and interstitium equilibrate. Longer descending limbs allow more time for water to flow out of the filtrate, so longer limbs make the filtrate more hypertonic than shorter limbs.
Ascending limb
Unlike the descending limb, the ascending limb of Henle’s loop is impermeable to water, a critical feature of the countercurrent exchange mechanism employed by the loop. The ascending limb actively pumps sodium out of the filtrate, generating the hypertonic interstitium that drives countercurrent exchange. In passing through the ascending limb, the filtrate grows hypotonic since it has lost much of its sodium content. This hypotonic
filtrate is passed to the distal convoluted tubule in the renal cortex.
Distal Convoluted Tubule (DCT)
The distal convoluted tubule is similar to the proximal convoluted tubule in structure and function. Cells lining the tubule have numerous mitochondria, enabling active transport to take place by the energy supplied by ATP. Much of the ion transport taking place in the distal convoluted tubule is regulated by the endocrine system. In the presence of parathyroid hormone, the distal convoluted tubule reabsorbs more calcium and excretes more phosphate. When aldosterone is present, more sodium is reabsorbed and more potassium excreted. Atrial natriuretic peptide causes the distal convoluted tubule to excrete more sodium. In addition, the tubule also secretes hydrogen and ammonium to regulate pH. After traveling the length of the distal convoluted tubule, only 3% of water remains, and the remaining salt content is negligible. 97.9% of the water in the glomerular filtrate enters the convoluted tubules and collecting ducts by osmosis.
Collecting ducts
Each distal convoluted tubule delivers its filtrate to a system of collecting ducts, the first segment of which is the connecting tubule. The collecting duct system begins in the renal cortex and extends deep into the medulla. As the urine travels down the collecting duct system, it passes by the medullary interstitium which has a high sodium concentration as a result of the loop of Henle’s countercurrent multiplier system. Though the collecting duct
is normally impermeable to water, it becomes permeable in the presence of antidiuretic hormone (ADH). As much as three-fourths of the water from urine can be reabsorbed as it leaves the collecting duct by osmosis. Thus the levels of ADH determine whether urine will be concentrated or dilute. Dehydration results in an increase in ADH, while water sufficiency results in low ADH allowing for diluted urine. Lower portions of the collecting duct are also permeable to urea, allowing some of it to enter the medulla of the kidney, thus maintaining its high ion concentration (which is very important for the nephron). Urine leaves the medullary collecting ducts through the renal papilla, emptying into the renal calyces, the renal pelvis, and finally into the bladder via the ureter. Because it has a different embryonic origin than the rest of the nephron (the collecting duct is from endoderm whereas the nephron is from mesoderm), the collecting duct is usually not considered a part of the nephron proper.
Renal Hormones
1. Vitamin D- Becomes metabolically active in the kidney. Patients with renal disease have symptoms of disturbed calcium and phosphate balance.
2. Erythropoietin- Released by the kidneys in response to decreased tissue oxygen levels (hypoxia).
3. Natriuretic Hormone- Released from cardiocyte granules located in the right atria of the heart in response to increased atrial stretch. It inhibits ADH secretions which can contribute to the loss of sodium and water.
Source: Cray MI, Ch. 8 The Urinary System ,Textbook of Human Physiology and Biophysics, V#1. Atlanta Ga: IVMS 2014:217-29
